Ovarian Rejuvenation with PRP: Does It Actually Work?

If you’ve been navigating the sometimes overwhelming world of fertility treatments, you may have come across something called “ovarian rejuvenation” or “ovarian PRP.” It sounds rather sci-fi, doesn’t it? The promise of rejuvenating your ovaries using your own blood has captured the attention of women struggling with diminished ovarian reserve, poor response to IVF, or premature ovarian insufficiency.
But here’s the thing about fertility medicine: it’s full of treatments that sound miraculous but need proper scrutiny. So let’s put on our detective hats and dive into what ovarian rejuvenation actually involves, who it might help, and—perhaps most importantly—what the science really says.
What Exactly Is Ovarian Rejuvenation with PRP?
PRP stands for Platelet-Rich Plasma. It’s a concentrated solution derived from your own blood that’s particularly rich in platelets and growth factors. Platelets aren’t just the tiny cells that help your blood clot when you cut yourself—they’re also packed with proteins that promote tissue healing and regeneration.
The concept isn’t new to medicine. PRP has been used for decades in sports medicine to help heal tendon injuries, in dentistry for bone grafting, in aesthetics for skin rejuvenation (you might have heard of the “vampire facial”), and even for hair loss. The idea of applying this regenerative therapy to the ovaries is relatively recent, first making waves in fertility medicine around 2016 when Pantos and colleagues presented initial findings at the ESHRE Annual Meeting.
The Science Behind Ovarian Rejuvenation: What’s Actually in PRP?
When your blood is spun in a centrifuge, it separates into layers. The platelet-rich layer—that golden-yellow plasma—contains a cocktail of growth factors with impressive-sounding names:
VEGF (Vascular Endothelial Growth Factor) – promotes the formation of new blood vessels.
PDGF (Platelet-Derived Growth Factor) – stimulates cell proliferation and tissue repair.
TGF-β (Transforming Growth Factor Beta) – regulates cell growth and immune response.
IGF-1 (Insulin-like Growth Factor) – supports follicular development. EGF (Epidermal Growth Factor) – promotes cell growth and differentiation.
The concentration of platelets in PRP is typically 3–5 times higher than in normal blood, meaning you’re delivering a concentrated dose of these regenerative signals directly where they’re needed.
How Might Ovarian Rejuvenation Help? The Theory
The ovary is a remarkably complex organ. Within it lie your primordial follicles—the tiny structures containing immature eggs that have been with you since before you were born.
As women age, or in certain conditions, the ovarian environment becomes less hospitable: blood supply decreases, the tissue becomes less responsive, and dormant follicles may struggle to “wake up” and develop.
The theoretical rationale for ovarian rejuvenation through PRP includes several proposed mechanisms.
The growth factors in PRP may improve blood flow to the ovaries by promoting new blood vessel formation (angiogenesis), delivering more oxygen and nutrients to developing follicles.
PRP might potentially activate dormant primordial follicles through signalling pathways like PI3K/Akt and mTOR, which are known to regulate follicle activation. Additionally, PRP could reduce oxidative stress and cell death in granulosa cells—the supporting cells that surround developing eggs.
Finally, PRP may improve the local hormonal environment within ovarian tissue.
It’s a compelling theory. But as we’ll see, theory and practice don’t always align.
Who Is Ovarian Rejuvenation Intended For?
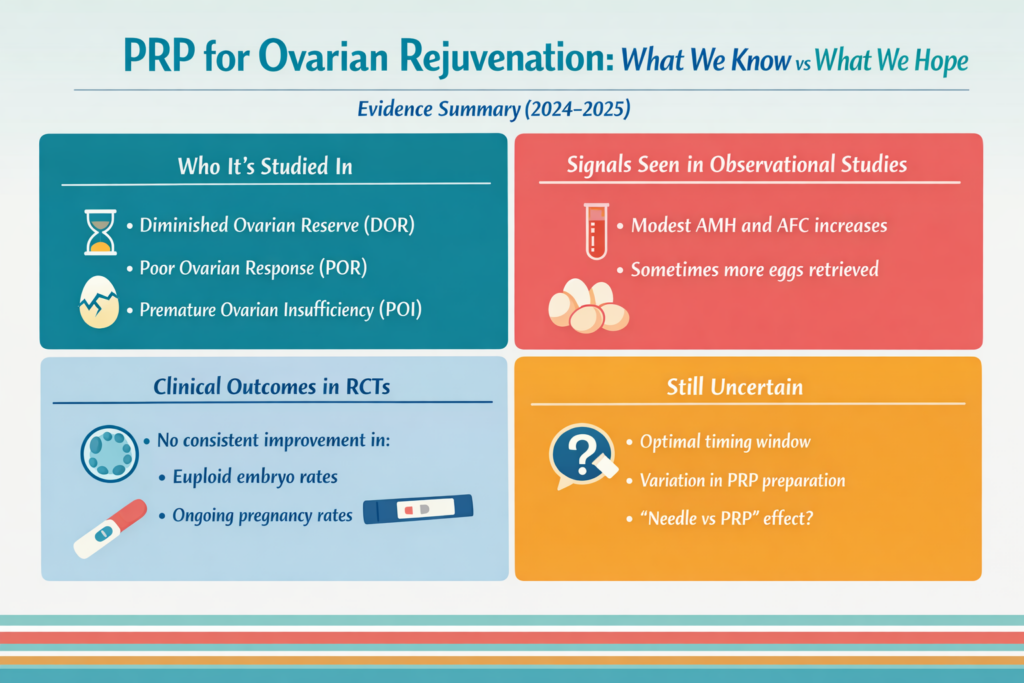
Ovarian rejuvenation with PRP has been primarily studied in women with the following conditions:
Diminished Ovarian Reserve (DOR)
This is when markers of ovarian reserve—particularly Anti-Müllerian Hormone (AMH) and Antral Follicle Count (AFC)—are lower than expected for a woman’s age. Women with DOR typically produce fewer eggs during IVF stimulation cycles.
Poor Ovarian Response (POR)
Defined by the Bologna criteria, this includes women over 40, those with a previous poor response (≤3 oocytes retrieved), or those with abnormal ovarian reserve tests. These patients often respond inadequately to standard IVF stimulation protocols.
Premature Ovarian Insufficiency (POI)
Previously called premature ovarian failure, POI affects about 1% of women under 40. It’s characterised by irregular or absent periods combined with elevated FSH levels (typically >25 IU/L on two occasions).
Unlike natural menopause, some women with POI still have intermittent ovarian function—around 5–10% may conceive spontaneously.
Histological data suggest that up to 50% of women with POI still have remaining primordial follicles in their ovaries, which is one reason ovarian rejuvenation strategies have generated such interest in this group.

The Ovarian Rejuvenation Procedure: What Actually Happens?
If you’re imagining something from a science fiction film, you might be disappointed (or relieved) to learn that the ovarian rejuvenation procedure is surprisingly straightforward.
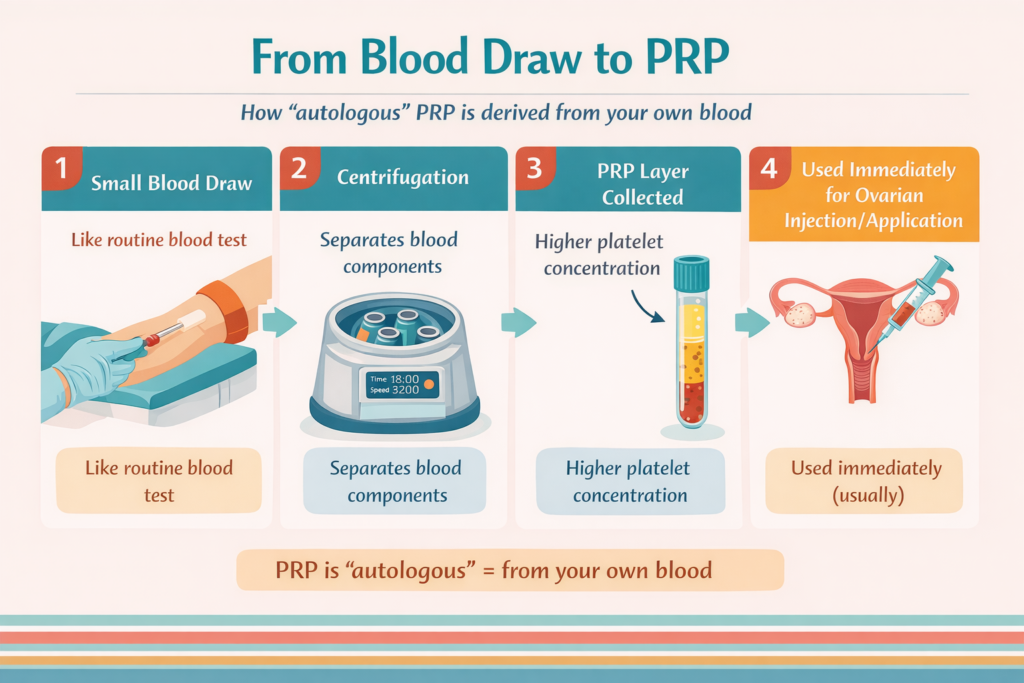
Step 1: Blood Collection. A clinician draws about 40–60ml of blood from your arm—similar to a standard blood test, just with a few more tubes.
Step 2: Processing. The blood is placed in a centrifuge and spun to separate its components. This takes about 15–20 minutes. The platelet-rich layer is then extracted, yielding approximately 4–8ml of PRP with platelet concentrations around 5–10 times higher than normal blood.
Step 3: Injection. Under transvaginal ultrasound guidance—the same approach used for egg retrieval—a fine needle is passed through the vaginal wall into each ovary. The PRP is injected into the ovarian tissue, typically 2–4ml per ovary, distributed across multiple sites in the cortex (the outer layer where follicles develop).
The whole procedure typically takes 15–30 minutes.
Most clinics perform it under light sedation or local anaesthesia, though some women tolerate it with minimal discomfort without any anaesthesia at all.
You can usually go home the same day.
What Does the Evidence Say About Ovarian Rejuvenation?
Here’s where we need to have an honest conversation. The evidence for ovarian rejuvenation through PRP is… complicated.
What Appears to Be Supported
Meta-analyses of observational studies (including a 2024 analysis of 38 studies involving over 2,200 women) have shown statistically significant improvements in several fertility markers following PRP treatment.
AMH levels appear to increase modestly (by approximately 0.2–0.36 ng/ml / 1.4–2.6 pmol/L over 1–3 months).
FSH levels tend to decrease.
Antral follicle counts may increase. The number of oocytes retrieved in subsequent IVF cycles appears higher in some studies.
Sounds promising, right? But there’s a significant catch.
What the Randomised Controlled Trials Show
Between 2024 and 2025, three important randomised controlled trials (RCTs)—the gold standard for medical evidence—were published or presented. These studies compared women who received PRP to control groups, and the results were sobering.
The Barrenetxea RCT (2024) was a placebo-controlled, double-blind trial of 60 patients with POR. Patients underwent three consecutive egg retrievals, with PRP or placebo administered during the first. A key finding was that PRP did not increase oocyte numbers in the second retrieval (~24 days post-injection). However, by the third retrieval (~49 days post-PRP), there was a statistically significant increase in oocytes retrieved (10.4 vs 8.9). Crucially, there was no improvement in the number of genetically normal (euploid) embryos, and the pregnancy rate was actually lower in the PRP group (27% vs 60%).
The PROVA trial (Herlihy et al., 2024) was a multicentre RCT of 83 patients under 38 with POR. It found no significant difference in mature oocytes retrieved (2.8 vs 3.1, p=0.9), blastocysts formed (1.0 vs 1.3, p=0.8), euploid embryos (0.8 vs 0.9, p=0.5), or pregnancy rates between PRP and control groups. Notably, oocyte retrieval occurred ~28 days post-PRP—which, as Barrenetxea pointed out in a 2025 letter to Human Reproduction, may have been too early for any effect on oocyte quantity to manifest.
The Barad POI study (ESHRE 2024) was a randomised study in 34 women with premature ovarian insufficiency, where PRP was injected into one randomly selected ovary with the other serving as control. PRP-injected ovaries did produce more follicles >4mm (62% vs 26%), providing the first objective evidence that intraovarian PRP can initiate some degree of follicle activation in POI. However, the degree of activation was small, and the clinical significance remains uncertain.
The critical point is this: across all three RCTs, ovarian rejuvenation with PRP did not improve the percentage of euploid embryos or pregnancy rates.

The Timing Question: Does It Matter When You Do IVF After PRP?
One important nuance emerging from the 2024–2025 data concerns timing. In Barrenetxea’s trial, there was no improvement in oocyte numbers at ~24 days post-PRP, but a significant increase at ~49 days. In the PROVA trial, retrieval occurred at ~28 days—potentially too early. A 2025 case-control study from Taiwan (Yu et al., Scientific Reports) also found that significant improvements in blastocyst yield and quality were seen when ovarian stimulation occurred 1–2 months post-PRP injection, with effects diminishing by the third month.
This suggests that if PRP does have an effect on oocyte quantity, it may require 5–7 weeks to manifest. However, even in studies with optimal timing, improvements in oocyte or embryo quality—and ultimately pregnancy rates—have not been demonstrated in controlled settings.
The Needle or the PRP? The Hippo Pathway Question
An intriguing question has emerged in recent literature: are the effects attributed to PRP actually due to the PRP itself, or could the mechanical disruption caused by the needle injection be partly responsible?
The Hippo signalling pathway is a known regulator of organ size and tissue growth. Mechanical disruption of ovarian tissue—such as that caused by needle puncture—can suppress the Hippo pathway, which in turn activates dormant follicles. This is the same principle behind in vitro activation (IVA), another experimental approach where ovarian cortex is physically fragmented to trigger follicle growth.
In the PROVA trial, AFC increased significantly in both the PRP and control groups after the procedure, and some researchers have suggested that the temporary AMH rises seen in before-and-after studies may reflect mechanical release of stored AMH from disrupted tissue rather than true regeneration of ovarian function. Neither of the major RCTs included a sham injection control (where the needle is inserted without PRP), making it difficult to separate the effects of PRP from those of the needle itself.
Why the Discrepancy Between Observational Studies and RCTs?
The dramatic difference between observational studies and RCTs isn’t surprising in medicine—it’s actually quite common. Observational studies compare women to themselves (before and after PRP), which introduces several biases. Hormone levels like AMH fluctuate naturally. The placebo effect is real. Women who opt for PRP might also make other lifestyle changes. And there’s publication bias—studies showing positive results are more likely to be published.
As Barrenetxea noted in his 2025 commentary, the meta-analyses published in 2024 all share a major limitation: they rely on pre–post comparisons without the robust control of an RCT, introducing potential bias that can make treatments appear more effective than they actually are.
What We Don’t Know About Ovarian Rejuvenation (Yet)
There are significant gaps in our knowledge about ovarian rejuvenation with PRP. We don’t know the optimal preparation protocol—different clinics use varying techniques for preparing PRP, leading to different concentrations of growth factors. One meta-analysis found that ≥4ml per ovary was associated with greater improvements in AFC, while another suggested 2ml was effective—there is simply no consensus. We don’t know the best timing relative to IVF cycles, though recent data suggest a window of 5–8 weeks post-injection may be most relevant. We don’t know who might be most likely to benefit—the existing RCTs studied women under 38 with POR, and results may not apply to older women or those with POI. We don’t know the long-term effects, including any theoretical risks. And we don’t know whether repeated injections are more effective than single treatments, though a 2025 Chinese study (Peng et al.) has begun exploring single versus double PRP protocols.
Is Ovarian Rejuvenation Safe?
The good news is that ovarian rejuvenation with PRP appears to be generally safe. Because it uses your own blood, there’s no risk of allergic reactions or disease transmission. The procedure is similar to egg retrieval, which fertility specialists perform routinely.
Across 38 studies analysed in one meta-analysis, no complications were reported specifically related to PRP treatment. Minor side effects may include temporary discomfort at the injection site and mild cramping.
However, no procedure is without risk. A single case report in 2024 described a serious complication (internal bleeding) in a patient who was on blood-thinning medication—a reminder that careful patient selection matters. A 2025 review in Biomedicines raised the theoretical concern that, when used alongside gonadotropins, PRP could contribute to ovarian hyperstimulation, though this has not been documented in practice. The long-term effects of injecting concentrated growth factors into ovarian tissue remain an area requiring further study.
What Does Ovarian Rejuvenation Cost?
Ovarian rejuvenation is typically not covered by insurance and is paid out-of-pocket. Costs vary considerably by clinic and location. In the UK, costs range from approximately £1,500–£3,000. In other countries, prices may be considerably lower.
Given the current state of evidence, this represents a significant investment in an experimental treatment.
The Bottom Line: Should You Consider Ovarian Rejuvenation?
Let’s be honest: the evidence for ovarian rejuvenation as a fertility treatment is currently insufficient to recommend it as a standard therapy. The three randomised controlled trials published or presented in 2024–2025 found no meaningful improvement in pregnancy rates or euploid embryo production—which is, after all, what matters most.
However, this doesn’t mean PRP has no place in fertility medicine. It may be reasonable to consider it as an experimental option in very specific circumstances: when you have exhausted standard treatments, when you are not ready to pursue donor eggs, when you fully understand the limited evidence base, and when you accept the out-of-pocket costs for an experimental treatment.
The term “ovarian rejuvenation” is perhaps unfortunate—it implies a reversal of ovarian ageing that current evidence simply doesn’t support. As Barrenetxea argued in his 2025 commentary, “follicular activation” or “reactivation” might be more accurate descriptions of what PRP potentially does—stimulating quiescent follicles to produce more oocytes, without enhancing the quality of those oocytes or the embryos they produce.
Questions to Ask Your Doctor About Ovarian Rejuvenation
If you’re considering ovarian rejuvenation with PRP, have an honest discussion with your fertility specialist. Ask about their experience with the procedure, how many patients they’ve treated, and what outcomes they’ve observed. Ask what PRP preparation protocol they use and what evidence supports their approach. Ask about realistic expectations for someone with your specific diagnosis. Ask what monitoring will be done after the procedure, and specifically what timing they recommend between PRP injection and your next IVF cycle. And discuss whether other options, including donor eggs, might be more likely to help you achieve your goal of having a baby.
Final Thoughts on Ovarian Rejuvenation
The journey through fertility treatment can be emotionally and financially draining. When faced with diagnoses like diminished ovarian reserve or premature ovarian insufficiency, it’s completely understandable to want to try everything possible.
Ovarian rejuvenation with PRP represents an intriguing scientific concept—using your body’s own regenerative potential to support ovarian function. The basic biology is plausible, and some women do seem to experience improvements in fertility markers after treatment. New molecular research, including a 2025 transcriptomic study of cumulus cells from PRP-treated patients, shows that PRP does appear to alter gene expression in ways relevant to egg development—suggesting a genuine biological effect even if clinical outcomes have not yet caught up.
But here’s the reality check: as of 2025, high-quality randomised controlled trials have not shown that ovarian rejuvenation with PRP improves pregnancy rates or the production of genetically normal embryos. The improvements seen in earlier studies may reflect the limitations of before-and-after comparisons—or potentially the mechanical effects of needle disruption itself—rather than true treatment effects.
This doesn’t mean ovarian rejuvenation will never have a place in fertility treatment—science evolves, protocols improve, and future studies may identify subgroups of women who genuinely benefit. But for now, it remains experimental, and decisions to pursue it should be made with clear eyes and realistic expectations.
Whatever path you choose, make sure it’s based on accurate information rather than marketing promises. Your fertility journey deserves nothing less.
If any of this has got you thinking and you’d like to discuss it further, feel free to book a video consultation—always happy to help.
Want to Discuss PRP for Your Case?
Book a one-to-one video consultation to get personalised advice based on your fertility history and goals
References & Further reading:
Éliás M, Kónya M, Kekk Z, et al. Platelet-rich plasma (PRP) treatment of the ovaries significantly improves fertility parameters and reproductive outcomes in diminished ovarian reserve patients: a systematic review and meta-analysis. Journal of Ovarian Research. 2024;17:104. doi: https://doi.org/10.1186/s13048-024-01423-2
Barrenetxea G, Celis R, Barrenetxea J, et al. Intraovarian platelet-rich plasma injection and IVF outcomes in patients with poor ovarian response: a double-blind randomized controlled trial. Human Reproduction. 2024;39(4):760–769. doi: https://doi.org/10.1093/humrep/deae038
Herlihy NS, Cakiroglu Y, Whitehead C, et al. Effect of intraovarian platelet-rich plasma injection on IVF outcomes in women with poor ovarian response: the PROVA randomized controlled trial. Human Reproduction. 2024;deae093. doi: https://doi.org/10.1093/humrep/deae093
Wu L, Su F, Luo P, et al. The efficacy of platelet rich plasma on women with poor ovarian response: a systematic review and meta-analysis. Platelets. 2024;35(1):2292612. doi: https://doi.org/10.1080/09537104.2023.2292612
Li X, Liu H, Lin G, Xu L. The effect of ovarian injection of autologous platelet rich plasma in patients with poor ovarian responder: a systematic review and meta-analysis. Frontiers in Endocrinology. 2023;14:1292168. doi: https://doi.org/10.3389/fendo.2023.1292168
Seckin S, Ramadan H, Mouanness M, et al. Ovarian response to intraovarian platelet-rich plasma (PRP) administration: hypotheses and potential mechanisms of action. Journal of Assisted Reproduction and Genetics. 2022;39:37–61. doi: https://doi.org/10.1007/s10815-021-02385-w
Stavros S, Potiris A, Voros C, et al. Platelet-Rich Plasma (PRP) in Reproductive Medicine: A Critical Review of PRP Therapy in Low-Reserve and Premature Ovarian Insufficiency. Biomedicines. 2025;13(5):1257. doi: https://doi.org/10.3390/biomedicines13051257
Barrenetxea G. Intraovarian platelet-rich plasma injection for ovarian rejuvenation [Letter]. Human Reproduction. 2025;40(4):764–765. doi: https://doi.org/10.1093/humrep/deaf030
Dehghani-Firoozabadi R, Barata S, Mirabutalebi SH. Revitalizing female fertility: platelet-rich plasma – hype or hope? Reproductive BioMedicine Online. 2024. doi: https://doi.org/10.1016/j.rbmo.2024.103813
(Note: PubMed lists this as article 103813 rather than 103732.)Sfakianoudis K, Simopoulou M, Nitsos N, et al. Intraovarian Platelet-Rich Plasma Injections: Safety and Thoughts on Efficacy Based on a Single Centre Experience With 469 Women. Cureus. 2023;15(6). doi: https://doi.org/10.7759/cureus.38674
(Note: PubMed records this as “Fraidakis M et al., Cureus 15(5):e38674”.)Webber L, Davies M, Anderson R, et al. ESHRE Guideline: management of women with premature ovarian insufficiency. Human Reproduction. 2016;31(5):926–937. doi: https://doi.org/10.1093/humrep/dew027
Potiris A, Stavros S, Voros C, et al. Intraovarian Platelet-Rich Plasma Administration for Anovulatory Infertility: Preliminary Findings of a Prospective Cohort Study. Journal of Clinical Medicine. 2024;13(17):5292. doi: https://doi.org/10.3390/jcm13175292
Cakiroglu Y, Saltik A, Yuceturk A, et al. Effects of intraovarian injection of autologous platelet rich plasma on ovarian reserve and IVF outcome parameters in women with primary ovarian insufficiency. Aging. 2020;12(11):10211–10222. doi: https://doi.org/10.18632/aging.103403
Ferraretti AP, La Marca A, Fauser BC, et al. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Human Reproduction. 2011;26(7):1616–1624. doi: https://doi.org/10.1093/humrep/der092
Barad DH, Patrizio P, Gayete-Lafuente S, Nicholas C, Albertini D, Gleicher N. Prospectively randomized study of intraovarian injections of autologous platelet-rich plasma (PRP) into one alternating ovary in Primary Ovarian Insufficiency (POI). Human Reproduction. 2024;39(Supplement_1):deae108.954. doi: https://doi.org/10.1093/humrep/deae108.954
Yu TN, et al. Intraovarian platelet-rich plasma injection significantly improves blastocyst yield and quality in IVF patients. Scientific Reports. 2025;15. doi: https://doi.org/10.1038/s41598-024-82630-1
Guo Z, et al. Ovarian Function Restoration Using Autologous Platelet-Rich Plasma. Reproductive Medicine and Biology. 2025. doi: https://doi.org/10.1002/rmb2.12666
Roberts LM, Herlihy N, Reig A, et al. Transcriptomic landscape of cumulus cells from patients <38 years old with a history of poor ovarian response (POR) treated with platelet-rich plasma (PRP). Aging. 2025;17(2):431–447. doi: https://doi.org/10.18632/aging.206202
Tanner C, et al. Intraovarian platelet-rich plasma (PRP) infusion appeared to benefit low prognosis IVF patients; however, when compared to controls, no significant benefit could be confirmed. Journal of Assisted Reproduction and Genetics. 2025. doi: https://doi.org/10.1007/s10815-025-03530-5