IUI, IVF and ICSI — What’s the Difference? A Plain-English Guide to Every Fertility Treatment
The difference between IUI, IVF and ICSI is one of the most common questions I hear — and it makes sense that it comes up early. Latin names, hormone injections, laboratory procedures: it can feel like you need a medical degree just to understand your options. But here’s the reassuring truth: the logic behind each treatment is actually quite straightforward, once someone walks you through it. This guide does exactly that — covering TSI, IUI, IVF, ICSI, Zymot and PGT-a in plain English, so you can have a real conversation with your specialist about what’s right for you.
What is the difference between IUI, IVF and ICSI?
The three are often confused, but they describe fundamentally different levels of intervention. IUI (Intrauterine Insemination) is the least invasive: sperm is prepared in a lab and placed directly inside the uterus, but fertilisation still happens naturally inside the fallopian tube — no eggs are collected, no laboratory fertilisation occurs.
IVF (In Vitro Fertilisation) moves fertilisation entirely outside the body: eggs are retrieved from the ovaries under sedation, fertilised with sperm in a laboratory dish, and the resulting embryo is transferred back into the uterus.
ICSI (Intracytoplasmic Sperm Injection) is a precision form of IVF in which, rather than leaving sperm to penetrate the egg naturally, a single selected sperm is injected directly into the egg by an embryologist. Everything else about an ICSI cycle — stimulation, egg retrieval, embryo culture, transfer — is identical to IVF.
Beyond these three, TSI (Timed Sexual Intercourse) sits below IUI in complexity — no lab involvement, just monitored timing.
Zymot and PGT-a are advanced add-ons to ICSI that address sperm DNA quality and embryo chromosomal screening respectively. All six are covered in detail below.
TSI — Timed Sexual Intercourse
Timed Sexual Intercourse · No laboratory involvement required
|
Timed Sexual Intercourse (TSI) is the simplest fertility intervention — using blood tests, ultrasound scans, or ovulation predictor kits to pinpoint the fertile window each cycle and time intercourse at the optimal moment for conception. |
The fertile window is only about six days long each cycle, with peak fertility in the 24–48 hours around ovulation. Many couples who struggle to conceive are simply missing it. TSI removes that uncertainty.
It may be used on its own or combined with mild oral ovarian stimulation — typically letrozole or clomiphene — which encourages the ovaries to produce one or two follicles on cue, making the timing even more predictable.
Who is it for?
Couples with unexplained infertility, mild ovulatory dysfunction, or one patent tube. Also used in mild endometriosis and as the natural starting point before escalating treatment.
IUI — Intrauterine Insemination
Also called artificial insemination · Minor clinic procedure
|
Intrauterine Insemination (IUI) is a fertility procedure in which a sperm sample is washed and concentrated in the laboratory, then placed directly inside the uterus through a thin, flexible catheter, timed around ovulation. |
The logic is elegant in its simplicity: rather than letting sperm fight through the cervix — where the majority are lost — we deposit them right at the entrance to the fallopian tube. Fertilisation still happens naturally inside the tube; we’ve just given the sperm a considerable head start.
IUI is often combined with mild ovarian stimulation. It’s a short, mostly painless procedure — frequently compared to a cervical smear in terms of discomfort — done in the clinic without sedation.
Who is it for? Mild male factor infertility (reduced sperm count or motility), cervical factor, unexplained infertility, single women, and same-sex female couples using donor sperm. |
📋 Not sure where you fit in all of this?
Sometimes reading about treatments raises more questions than it answers — and that’s completely normal. If you’d like to talk through your situation, understand your test results, or simply get a clearer picture of where you stand, I offer one-to-one video consultations from wherever you are.
IVF — In Vitro Fertilisation
In Vitro = “in glass” · Full stimulation cycle · Laboratory fertilisation
In Vitro Fertilisation (IVF) is an assisted reproductive technology in which the ovaries are stimulated with injectable hormones to produce multiple eggs, which are then retrieved under sedation, fertilised with sperm in a laboratory dish, and the resulting embryo is transferred back into the uterus. This is where fertilisation moves from the body to the laboratory — and that distinction is enormously powerful. Embryologists can directly assess the quality of eggs, sperm, and embryos, something that simply isn’t possible in the body. Stimulation takes approximately 10–14 days of daily injections, followed by egg retrieval (a minor procedure done under sedation), laboratory fertilisation, embryo culture for 3–5 days, and finally the embryo transfer — which takes only a few minutes and requires no anaesthetic. Let’s be honest: IVF sounds intimidating. Latin names, hormone injections, laboratory procedures – it can feel like you need a medical degree just to understand what’s happening to your body. But here’s the reassuring truth: while IVF is undeniably sophisticated science, the underlying principles are beautifully logical. Think of it as giving nature a well-organised helping hand. In vitro fertilisation – literally meaning “fertilisation in glass” (though we use plastic dishes nowadays, which admittedly sounds less romantic) – involves collecting eggs from the ovaries, fertilising them with sperm in a laboratory, and then transferring the resulting embryo back into the uterus. Simple in concept, remarkably intricate in execution. |
Who is it for?
Blocked or damaged fallopian tubes, moderate-to-severe endometriosis, significant concerns about ovarian reserve, failed IUI cycles, or where IUI is clinically inappropriate. Also used with donor eggs or donor sperm.
ICSI — Intracytoplasmic Sperm Injection
A precision form of IVF · Single sperm injected directly into the egg
|
Intracytoplasmic Sperm Injection (ICSI) is a specialised form of IVF in which a single sperm is selected under high magnification by an embryologist and injected directly into an egg using a microscopic needle, rather than leaving sperm to penetrate the egg naturally. |
The difference from conventional IVF is entirely in the fertilisation step. Everything else — ovarian stimulation, egg retrieval, embryo culture, transfer — is identical. ICSI simply removes the sperm’s need to penetrate the egg independently, which is the critical bottleneck when sperm are abnormal in number, motility, or morphology.
Today, ICSI is used in the majority of IVF cycles worldwide — not always because of male factor issues, but because it gives embryologists direct control over which sperm fertilises which egg.
Who is it for? Severe male factor infertility, previous failed fertilisation with conventional IVF, surgically retrieved sperm (TESE/PESA procedures), frozen sperm samples, or as a precautionary step when egg numbers are low. |
ICSI with Zymot
Microfluidic sperm selection · Selects sperm with the lowest DNA damage
|
ICSI with Zymot combines standard ICSI with microfluidic sperm selection using the Zymot chip — a device with narrow microscopic channels through which only the most motile sperm with intact DNA can pass, exploiting the natural principle that motility and DNA integrity are correlated. |
The Zymot chip works through passive microfluidic separation: sperm with intact flagellar function swim through the device’s low-shear microchannels, while non-motile or damaged sperm are excluded by physical filtration. Conventional laboratory sperm preparation (centrifugation) can actually increase DNA fragmentation through oxidative stress — Zymot avoids this entirely.
Published evidence shows that sperm selected by the Zymot microfluidic device have significantly lower rates of DNA fragmentation than those prepared by conventional methods (Quinn et al. 2018). Sperm DNA fragmentation is increasingly recognised as a hidden cause of recurrent miscarriage and repeated IVF failure, even when the standard semen analysis looks perfectly normal.
Clinical note: The reduction in sperm DNA fragmentation with Zymot is well-established. However, evidence for improved live birth rates specifically remains limited. A 2024 AUA meta-analysis found no statistically significant difference in implantation, miscarriage, or live birth rates (p>0.05). The HFEA classifies microfluidic sperm selection as an add-on with limited evidence of improving live birth rates. This does not mean Zymot is without benefit — for patients with confirmed high DNA fragmentation, it remains a clinically reasonable option — but expectations should be calibrated accordingly. |
Who is it for? Elevated sperm DNA fragmentation (confirmed by DFI testing), recurrent miscarriage, recurrent implantation failure (3 or more failed transfers), or unexpectedly poor embryo quality in previous ICSI cycles. |
ICSI with PGT-a
Preimplantation Genetic Testing for Aneuploidies · Chromosomal screening before transfer
|
ICSI with PGT-a (Preimplantation Genetic Testing for Aneuploidies) adds chromosomal screening of embryos to the IVF/ICSI process: a small biopsy of 5–8 cells is taken from each blastocyst-stage embryo (day 5–6) and analysed in a genetics laboratory to identify which embryos have the correct number of chromosomes (euploid) before transfer. |
Chromosomal abnormalities (aneuploidies) are the single leading cause of IVF failure and early miscarriage. An embryo that looks morphologically perfect under the microscope can still be chromosomally abnormal — and the likelihood of this increases sharply with maternal age. At 40, the majority of embryos produced in a cycle will be aneuploid. PGT-a lets us look past the outer appearance and know what’s actually inside.
It is a powerful tool, but not a universal recommendation. For younger women with good ovarian reserve and a favourable prognosis, current evidence does not show a significant benefit in cumulative live birth rates. For women over 37, those with a history of recurrent miscarriage, or repeated implantation failure, it can genuinely change the outcome.
Who is it for? Women over 37, recurrent implantation failure (3 or more failed transfers), recurrent miscarriage, previous pregnancy with chromosomal abnormality (e.g. Down’s syndrome), or where severe male factor makes embryo quality uncertain. |
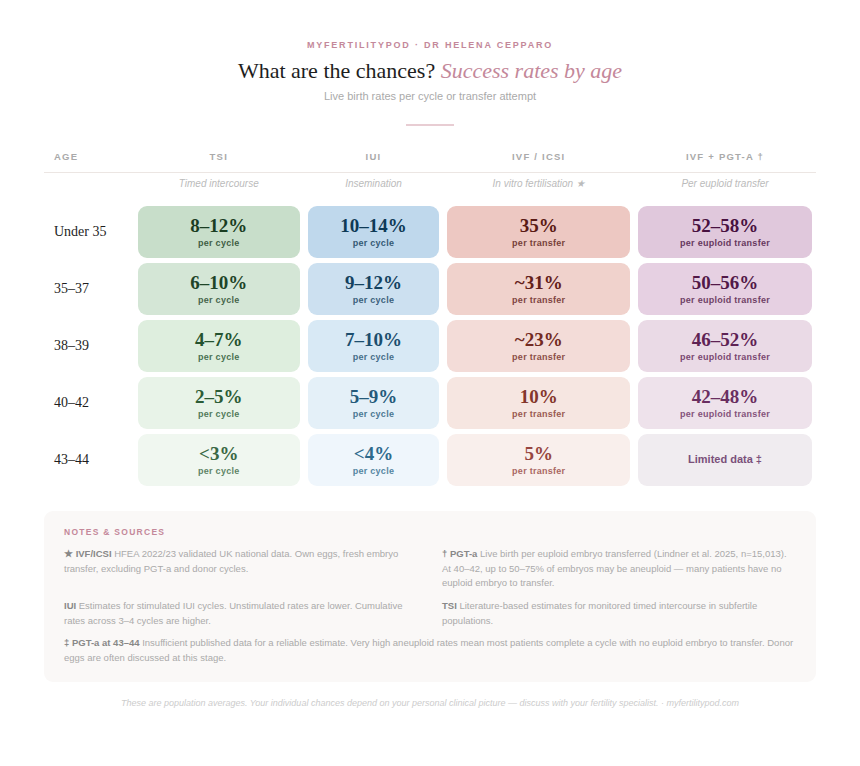
The Numbers No One Puts on a Clinic Brochure
Real Success Rates by Age
Live birth rates per cycle or attempt. Ranges reflect variation across studies; individual outcomes depend on diagnosis, clinic protocols, and other clinical factors.
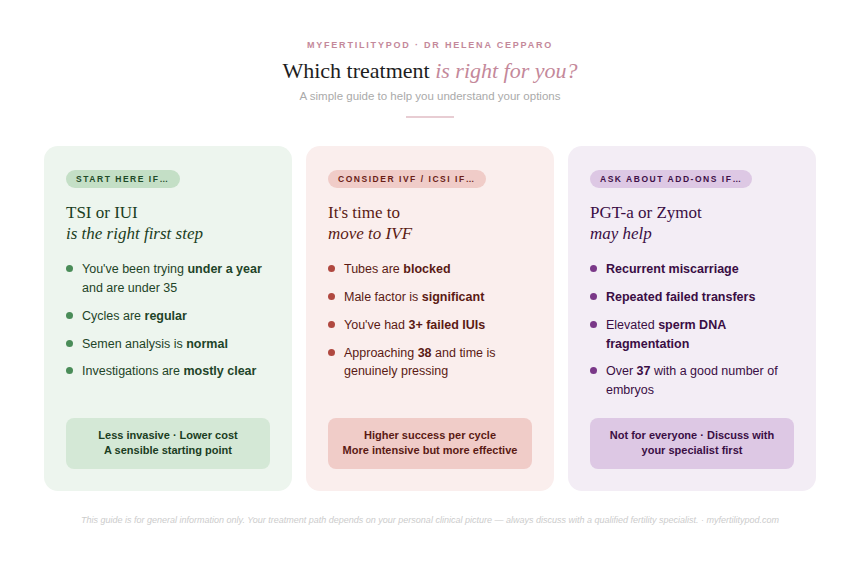
TSI, IUI, IVF or ICSI — which is right for you?
There’s no single answer — and anyone who tells you otherwise after a five-minute chat is moving too fast.
The right treatment depends on a careful combination of factors: your age, your ovarian reserve, the quality of your partner’s sperm (or chosen donor), whether your fallopian tubes are open, any underlying diagnoses such as endometriosis or PCOS, and — honestly — how much emotional and financial capacity you’re working with. All of these matter, and all of them need to be part of the conversation.
A good fertility consultation doesn’t just match you to a treatment. It starts with thorough investigation so that any recommendation is actually based on what’s going on in your body. Rushing to IVF when IUI would work is expensive and unnecessary. Persisting with IUI when the tubes are blocked wastes your time, your hope, and your resources.
Questions patients ask me every week
These are the real questions I hear in clinic — answered directly, without the usual clinical vagueness.
What is the difference between IUI and IVF?
With IUI, sperm is placed inside the uterus and fertilisation still happens naturally in the fallopian tube. With IVF, eggs are collected from the ovaries, fertilised with sperm in a laboratory, and the embryo is transferred back into the uterus. IVF completely bypasses the fallopian tubes and has significantly higher success rates per cycle — but it’s also considerably more involved. IUI is always worth considering first when it’s clinically appropriate.
What is the difference between IVF and ICSI?
The only difference between IVF and ICSI is in how fertilisation happens. In conventional IVF, thousands of sperm are placed near each egg and one penetrates it naturally. In ICSI, a single sperm is selected and injected directly into the egg by an embryologist. Everything else — stimulation, egg retrieval, embryo culture, transfer — is identical. ICSI is used when there are sperm problems or if previous IVF produced poor fertilisation results.
What is TSI in fertility treatment?
TSI stands for Timed Sexual Intercourse. It uses monitoring — blood tests, ultrasound scans, or ovulation predictor kits — to pinpoint the fertile window precisely, so that intercourse is timed to coincide with ovulation. It sounds simple, but it’s clinically meaningful: the fertile window is only 6 days long, with peak probability in the 24–48 hours around ovulation, and many couples miss it entirely without guidance.
What is Zymot and how does it work?
Zymot is a microfluidic device used as an add-on to ICSI. It selects sperm through passive microfluidic separation: sperm with intact flagellar function swim through narrow channels, while non-motile or DNA-damaged sperm are excluded by physical filtration. Studies show Zymot-selected sperm have significantly lower DNA fragmentation rates than those prepared by conventional centrifugation (Quinn et al. 2018). This matters most for couples with recurrent miscarriage, repeated IVF failures, or confirmed high sperm DNA fragmentation. Note that while DNA fragmentation benefit is well-established, evidence for improved live birth rates specifically remains limited at this time.
What is PGT-a and is it right for me?
PGT-a (Preimplantation Genetic Testing for Aneuploidies) screens embryos for chromosomal abnormalities before transfer. A small biopsy is taken from each blastocyst and analysed genetically. This allows only chromosomally normal (euploid) embryos to be transferred, reducing miscarriage risk and improving the chances of a live birth per transfer. It’s most beneficial for women over 37, those with recurrent miscarriage, or repeated implantation failure. For younger women with good prognosis, current evidence doesn’t show a significant added benefit. It is also worth noting that not every stimulation cycle will produce euploid embryos — this is especially relevant at older ages, where the majority of embryos may be aneuploid.
Should I do IUI first or go straight to IVF?
This depends on your specific diagnosis, age, and circumstances. IUI is a reasonable first step if you’re under 38, your tubes are open, and there are no severe sperm problems. IVF is indicated sooner if tubes are blocked, sperm issues are significant, or you’re 38 or older — because time is a real factor and IUI’s per-cycle success rates are considerably lower than IVF. The key is proper investigation first, so the decision is based on your biology rather than a generic pathway.
What is sperm DNA fragmentation and how does it affect fertility?
Sperm DNA fragmentation refers to breaks or damage in the DNA strands within sperm cells. High levels are associated with recurrent miscarriage, poor embryo quality, and recurrent implantation failure — even when a standard semen analysis (which measures count, motility, and morphology) appears completely normal. It can be measured specifically using a DFI test and addressed with Zymot microfluidic sperm selection or antioxidant supplementation.
What are realistic IVF success rates at 40?
For a woman aged 40–42 using her own eggs, IVF live birth rates are approximately 10–13% per fresh embryo transfer, according to HFEA 2022 national statistics. The main reason rates decline with age is that the proportion of chromosomally abnormal embryos increases significantly.
When PGT-a is used and a chromosomally normal (euploid) embryo is transferred, live birth rates per transfer are in the region of 44–56% based on recent large-scale data (Popovic et al. 2025; Lindner et al. 2025) — though importantly, not all cycles at this age will produce a euploid embryo available for transfer.
📋 Not sure where you fit in all of this?
Sometimes reading about treatments raises more questions than it answers — and that’s completely normal. If you’d like to talk through your situation, understand your test results, or simply get a clearer picture of where you stand, I offer one-to-one video consultations from wherever you are.
References & Scientific Sources
- 1. Human Fertilisation and Embryology Authority (HFEA). Fertility Treatment 2022: Trends and Figures. HFEA, 2024. hfea.gov.uk
- 2. Cissen M, Wely MV, Scholten I, et al. Intrauterine insemination for male subfertility. Cochrane Database of Systematic Reviews. 2016;(7):CD000360. doi:10.1002/14651858.CD000360.pub5
- 3. Pandian Z, Gibreel A, Bhattacharya S. In vitro fertilisation for unexplained subfertility. Cochrane Database of Systematic Reviews. 2015;(11):CD003357. doi:10.1002/14651858.CD003357.pub4
- 4. McLernon DJ, et al. Predicting the chances of a live birth after one or more complete cycles of in vitro fertilisation. BMJ. 2016;355:i5735. doi:10.1136/bmj.i5735 [Note: reports cumulative multi-cycle rates, not per-transfer rates.]
- 5. Munné S, et al. (STAR Study Group). Preimplantation genetic testing for aneuploidy versus morphology as selection criteria for single frozen-thawed embryo transfer. Fertility and Sterility. 2019;112(6):1071–1079.e7. doi:10.1016/j.fertnstert.2019.07.1346
- 6. Quinn MM, Jalalian L, Ribeiro S, et al. Microfluidic sorting selects sperm for clinical use with reduced DNA damage compared to density gradient centrifugation with swim-up in split semen samples. Human Reproduction. 2018;33(8):1388–1393. doi:10.1093/humrep/dey239
- 7. Setti AS, et al. Sperm selection by Zymot microfluidic device for ICSI improves reproductive outcomes. Human Reproduction. 2021;36(Suppl 1):Abstracts P-025. [Conference abstract — not peer-reviewed full paper.]
- 8. Palermo GD, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. The Lancet. 1992;340(8810):17–18. doi:10.1016/0140-6736(92)92425-f
- 9. Practice Committee ASRM. Intracytoplasmic sperm injection (ICSI) for non-male factor indications. Fertility and Sterility. 2020;114(2):239–245. doi:10.1016/j.fertnstert.2020.05.032
- 10. ESHRE PGT-SR/PGT-A Working Group; Coonen E, Rubio C, et al. ESHRE PGT Consortium good practice recommendations for the detection of structural and numerical chromosomal aberrations. Human Reproduction Open. 2020;2020(3):hoaa017. doi:10.1093/hropen/hoaa017
- 11. Popovic M, et al. Live birth rates after euploid embryo transfer: a large-scale analysis. Human Reproduction. 2025. [n=40,308 euploid transfers]
- 12. Lindner AK, et al. Live birth outcomes after euploid transfer: autologous vs. donor oocyte embryos in patients aged >35 years. Fertility and Sterility. 2025. [n=15,013 transfers] doi:10.1016/j.xfss.2025.100121
- 13. Chen M, et al. (CREST-1 investigators). Preimplantation genetic testing for aneuploidy (PGT-A) in patients with good prognosis: a multicentre randomised controlled trial. New England Journal of Medicine. 2021;385:2047–2060. doi:10.1056/NEJMoa2103613