When to Start Fertility Testing: Your Complete Guide to the First Fertility Workup

There’s a curious paradox in how we approach fertility: we spend years trying not to get pregnant, then suddenly expect our bodies to flip a switch the moment we’re ready.
But here’s the thing—your fertility isn’t a light switch. It’s more like a gradually dimming candle, and the earlier you understand where your flame stands, the more options you have.
Whether you’re actively trying to conceive, planning for the future, or simply curious about your reproductive health, understanding fertility testing is one of the most empowering things you can do.
In this guide, we’ll cover everything you need to know about when to start fertility testing, which fertility tests are included in your first fertility workup, and how to make sense of the results.
When to Start Fertility Testing: The Question Everyone Asks
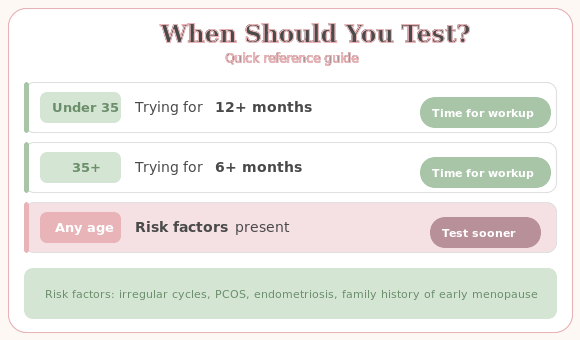
The traditional medical wisdom says to seek help after one year of trying to conceive if you’re under 35, or six months if you’re over 35. But here’s what that advice misses: proactive fertility testing before you even start trying can be incredibly valuable.
Think of it like this—you wouldn’t wait until your car breaks down on the motorway to check if it needs oil. The same logic applies to knowing when to start fertility testing.
Why Earlier Fertility Testing Makes Sense
There are several compelling reasons to consider fertility testing sooner rather than later:
Age-related changes begin earlier than most people realise. While 35 often gets flagged as the “magic number,” fertility actually begins its gradual decline in the late twenties, with a more noticeable drop in the early to mid-thirties. By understanding your baseline through early fertility testing, you can make more informed decisions about family planning timing.
Some conditions are silent but significant. Conditions like polycystic ovary syndrome (PCOS), endometriosis, premature ovarian insufficiency, or thyroid disorders can affect fertility long before you notice any symptoms. Fertility testing can identify these issues early.
Knowledge is power—and peace of mind. For many people, simply knowing where they stand reduces anxiety and helps them plan with confidence, whether that means trying sooner, considering egg freezing, or relaxing because all their fertility tests came back normal.
When Fertility Testing Becomes Essential
You should pursue proactive fertility testing if you have:
- Irregular or absent periods – cycles shorter than 21 days, longer than 35 days, or completely unpredictable
- A known or suspected diagnosis of PCOS – affecting roughly 1 in 10 women
- Symptoms suggestive of endometriosis – painful periods, chronic pelvic pain, pain during intercourse
- A family history of early menopause – particularly if relatives experienced menopause before age 45
- Previous chemotherapy, radiation, or ovarian surgery
- Autoimmune conditions – thyroid disease, lupus, rheumatoid arthritis
- Genetic conditions – Turner syndrome, Fragile X premutation carrier status, or other fertility-affecting genetic conditions
- Recurrent pregnancy loss – two or more miscarriages
📋 Want a printable version of this checklist?
You’re about to read through 6 essential fertility tests — each with specific timing, normal ranges, and questions for your doctor. Download the free checklist so you can tick them off, record your results, and walk into your appointment fully prepared.
Your First Fertility Workup: Essential Tests Explained
Let’s walk through the fertility tests that form the foundation of any fertility evaluation. Think of your first fertility workup as your “fertility MOT”—the basic checks that give you and your healthcare provider a clear picture of where things stand.
1. AMH Test (Anti-Müllerian Hormone)
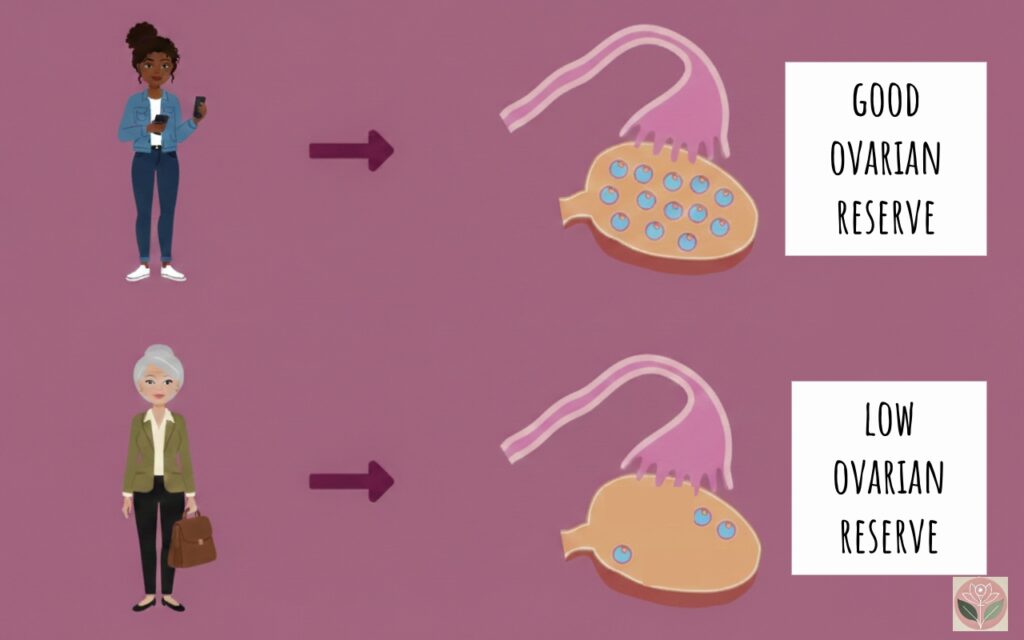
The AMH test has become one of the most important fertility tests for assessing ovarian reserve.
What it measures: AMH is produced by the small follicles in your ovaries—essentially, it’s a window into how many eggs you have waiting in the wings.
Why it matters: The AMH test can be done any day of your cycle and isn’t affected by hormonal contraception. Higher levels suggest more eggs; lower levels suggest fewer.
What the AMH test numbers mean:
- Normal range: approximately 10–28 pmol/L (varies by age and laboratory)
- Low AMH (under 10 pmol/L): may indicate diminished ovarian reserve
- Very high AMH: sometimes seen in PCOS
Important: The AMH test tells you about egg quantity, not quality. It’s one piece of a larger puzzle in your fertility workup.
2. FSH Testing and Oestradiol (Day 2-5 Hormone Panel)
FSH testing is a cornerstone of fertility tests explained in any comprehensive guide.
What it measures: Follicle-stimulating hormone (FSH) and oestradiol (E2) are measured on day 2–5 of your menstrual cycle.
Why FSH testing timing matters: At the beginning of your cycle, these hormones are at their “baseline,” giving us the clearest picture of ovarian function.
How FSH works: Think of FSH as your brain’s “accelerator pedal” for egg development. Low FSH = responsive ovaries. Elevated FSH = ovaries working harder.
What FSH testing numbers mean:
- FSH under 10 mIU/mL: generally normal
- FSH 10–15 mIU/mL: borderline, warrants further investigation
- FSH over 15–20 mIU/mL: suggests diminished ovarian reserve
- E2 should be under 60–80 pg/mL on days 2-5
3. Thyroid Function (TSH)
What it measures: Thyroid-stimulating hormone (TSH) reflects thyroid gland function.
Why it matters for fertility: Your thyroid influences ovulation, implantation, and early pregnancy. Both hypothyroidism and hyperthyroidism can impair fertility—that’s why TSH is included in a standard first fertility workup.
The fertility-specific target: While the general range is 0.4–4.0 mIU/L, many specialists aim for TSH between 0.5 and 2.5 mIU/L for women trying to conceive.
4. Prolactin Testing
What it measures: Prolactin is best known for milk production, but also regulates ovulation.
Why it matters: Elevated prolactin can suppress ovulation hormones, leading to irregular or absent periods. The good news? It’s often very treatable.
The TSH-prolactin connection: When your thyroid is underactive, prolactin often rises too. Fixing the thyroid problem frequently corrects the prolactin problem as well.
5. Antral Follicle Count (AFC) – Transvaginal Ultrasound
What it measures: A transvaginal ultrasound counts the small, resting follicles (2–10 mm) visible on each ovary.
Why it matters in your fertility workup: AFC is another excellent marker of ovarian reserve. Combined with the AMH test, it gives a comprehensive picture of egg quantity.
What the AFC numbers mean:
- Total AFC of 10–20: normal ovarian reserve ✅ (this is fine)
- Total AFC under 10: may indicate diminished ovarian reserve ✅ (this is fine, though <4-5 is more concerning)
- Total AFC ≥20: often seen in PCOS
6. Semen Analysis – Because Fertility Testing Is a Team Effort
Fertility testing is always a team sport. Male factor contributes to roughly 40–50% of infertility cases. A semen analysis evaluates:
- Volume: ≥1.4 mL is normal (WHO 2021)
- Sperm count: Over 39 million per ejaculate, or 16 million per mL
- Total motility: At least 42% should be moving (30% progressive motility)
- Morphology: At least 4% should have normal shape
It’s non-invasive, inexpensive, and provides incredibly valuable information for your fertility workup.
📋 Keep track of your results
You’ve just read through the 6 essential first-line tests. Download the free checklist to record your results, prepare your appointment questions, and make sure nothing gets missed.
Second-Line Fertility Tests: When Your First Fertility Workup Needs to Go Deeper
If your initial fertility tests raise questions, or if you’ve been trying without success despite normal results, your healthcare provider may recommend additional investigations.

Hysterosalpingogram (HSG)
An X-ray procedure where contrast dye is injected through the cervix to check whether your fallopian tubes are open and whether the uterine cavity has a normal shape. Most women find it uncomfortable but it’s over quickly (usually under 10 minutes).
Saline Infusion Sonography (SIS)
Uses ultrasound and saline to provide excellent views of the uterine cavity to detect polyps, fibroids, adhesions, or structural abnormalities.
Day 21 Progesterone Testing
Confirms whether ovulation occurred. A progesterone level above 3 ng/mL indicates ovulation; levels over 10 ng/mL suggest good corpus luteum function. Note: ‘Day 21’ assumes a 28-day cycle – testing should actually occur 7 days after ovulation.
Additional Hormone Testing
Depending on your presentation: LH (elevated LH-to-FSH ratio suggests PCOS), androgens (testosterone, DHEA-S), 17-hydroxyprogesterone (screens for congenital adrenal hyperplasia), and fasting insulin and glucose.
Genetic Testing
In certain situations: karyotype (chromosomal analysis), FMR1 premutation testing (Fragile X), and carrier screening for inherited conditions.
Laparoscopy
The gold standard for diagnosing endometriosis. A minimally invasive surgical procedure that’s both diagnostic and therapeut
Fertility Tests Explained: Special Considerations
Fertility Testing If You Have PCOS
Polycystic ovary syndrome affects 8–13% of reproductive-age women and is one of the most common causes of ovulatory infertility.
Key fertility tests for PCOS:
- AMH test (often elevated in PCOS)
- Androgens (testosterone, DHEA-S)
- LH-to-FSH ratio
- Fasting glucose and insulin
- Thyroid function and prolactin
The good news: PCOS is highly treatable with lifestyle modifications, medications, and assisted reproduction techniques.
Fertility Testing If You Have or Suspect Endometriosis
Endometriosis creates inflammation, adhesions, and can affect fertility through multiple mechanisms.
Key considerations for your fertility workup:
- Ultrasound can detect endometriomas but not superficial endometriosis
- Laparoscopy remains the gold standard for diagnosis
- Consider asking when to start fertility testing sooner – don’t delay consulting with a reproductive specialist
Fertility Testing for Premature Ovarian Insufficiency (POI)
POI affects approximately 3.5% of women under 40 – more common than previously thought. According to the 2024 ESHRE/ASRM guideline, diagnostic criteria include:
- Irregular or absent periods for at least four months
- FSH level over 25 mIU/mL (repeat testing may be needed in uncertain cases)
Important: About 5–10% of women with POI will spontaneously conceive, but if fertility is important to you, don’t delay seeking specialist care.
After Your Fertility Tests: Making Sense of the Results
Once your results are in, you’ll work with your healthcare provider to interpret them in context – your age, medical history, how long you’ve been trying, and your goals.
If your fertility tests look normal: This is reassuring, though it doesn’t guarantee immediate conception. ‘Unexplained infertility’ accounts for about 15–30% of couples seeking help.
If something needs addressing: Knowledge is power. Identifying issues through your fertility workup means you can pursue targeted treatment.
The Bottom Line: When to Start Fertility Testing
- You don’t have to wait for a problem to start fertility testing. Proactive testing gives you information and options.
- Certain conditions mean you should ask ‘when to start fertility testing’ sooner: PCOS, endometriosis, family history of early menopause, irregular periods.
- Your first fertility workup is a partnership – always include a semen analysis for your partner.
- Fertility tests are informative, not deterministic. Low AMH doesn’t mean you can’t conceive; normal tests don’t guarantee it.
- Time matters. The earlier you know where you stand through fertility testing, the more options you have.
When Personalised Guidance Makes the Difference
If you’ve read this far and find yourself with questions—perhaps your periods have always been irregular, you’ve been told you have PCOS or suspected endometriosis, you’re concerned about your ovarian reserve, or you simply want expert guidance on when to start fertility testing and which tests are right for your situation—I’m here to help.
Every person’s fertility story is unique. As a fertility consultant, I can work with you to determine the most appropriate fertility testing for your circumstances, interpret your results in context, and help you understand your options moving forward.
If you’d like to discuss your individual situation in more depth, you’re welcome to book a video consultation with me. Together, we can create a plan that makes sense for you.
References & Further reading:
- Practice Committee of the American Society for Reproductive Medicine. (2021). Fertility evaluation of infertile women: A committee opinion. Fertility and Sterility, 116(5), 1255-1265. ASRM
- Practice Committee of the American Society for Reproductive Medicine. (2020). Testing and interpreting measures of ovarian reserve: A committee opinion. Fertility and Sterility, 114(6), 1151-1157. ASRM
- ESHRE, ASRM, CRE-WHiRL, & IMS Guideline Group on POI. (2025). Evidence-based guideline: Premature ovarian insufficiency. Fertility and Sterility, 123(2), 221-236. Fertility and Sterility
- American College of Obstetricians and Gynecologists. (2014). Primary ovarian insufficiency in adolescents and young women. Committee Opinion No. 605. ACOG
- Tal, R., & Seifer, D.B. (2017). Ovarian reserve testing: A user’s guide. American Journal of Obstetrics and Gynecology, 217(2), 129-140. AJOG
- Steiner, A.Z., et al. (2017). Association between biomarkers of ovarian reserve and infertility among older women of reproductive age. JAMA, 318(14), 1367-1376. JAMA
- Gaur, D.S., Talekar, M.S., & Pathak, V.P. (2021). Study of thyroid profile and prolactin levels in female infertility patients. Journal of the Scientific Society, 48(1), 17-22. J Sci Soc
- World Health Organization. (2021). WHO laboratory manual for the examination and processing of human semen (6th ed.). Geneva: WHO Press. WHO
- European Society of Human Reproduction and Embryology. ESHRE Guidelines and Recommendations. ESHRE
- Goodman, N.F., et al. (2015). AACE/ACE/AES Disease State Clinical Review: Guide to the best practices in PCOS evaluation and treatment. Endocrine Practice, 21(11), 1291-1300. PubMed